
Inflammatory bowel disease (or IBD) is a group of chronic idiopathic, relapsing and remitting disorders that cause inflammation of the gastrointestinal tract.1–3Although it was traditionally regarded as a disease of westernised nations, IBD is becoming a global disease at the turn of the 21st century.2 It impacts every aspect of the affected individual's life4 and accounts for substantial costs to the health care system and society.4
Over 3.5 million people affected in the Western world

The prevalence of IBD in the Western world is up to 0.5% of the general population2
- Ng SC, et al. Lancet. 2018;390(10114):2769–2778.
- Kaplan, GG. Nat Rev Gastroenterol Hepatol. 2015;12:720–727.

The types of IBD and risk factors
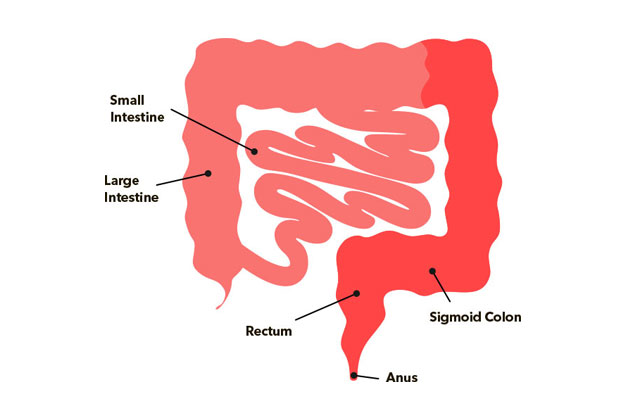
There are two main types of IBD: ulcerative colitis (UC) and Crohn’s disease (CD).5 Ulcerative colitis is a predominantly mucosal disease, its fundamental symptoms is rectal bleeding, and involves the rectum and can affect part of the colon or the entire colon in a continuous pattern.6 In contrast, Crohn’s disease can affect any part of the gastro-intestinal track (from mouth to rectum), although its location more common is the ileum.
Multifactorial Disease
Imbalance of Intestinal Microbiota Causitive & aggravating factors

- Khor B, et al. Nature. 2011;474(7351):307–317.
- Russell R. Postgrad Med J. 2001;77(904):82–88.
- Bjarnason I, et al. Pharmacol Ther. 1994;62(1–2):145–157.
- Mokhtarifar A, et al. Middle East J Dig Dis. 2013;5(2):93–97.
- Ni J, et al. Nat Rev Gastroenterol Hepatol. 2017;14(10):573–584.
- Ananthakrishnan AN, et al. Nat Rev Gastroenterol Hepatol. 2018;15(1):39–49
Although, ulcerative colitis and Crohn’s disease differ in location and depth of inflammation, they share similar symptoms.7 In general, the symptoms depend on the segment of the intestinal tract involved.8 Symptoms related to inflammatory damage in the gastrointestinal tract include diarrhoea (characterised by stools with mucus or blood, nocturnal diarrhoea or incontinence), constipation, pain or rectal bleeding with bowel movement, bowel movement urgency, tenesmus, abdominal cramps and pain, nausea and vomiting.8,9 If you have IBD you are at higher risk of also having iron deficiency and iron deficiency anaemia. Indeed, anaemia is the most common non-intestinal symptom of IBD10.
Ulcerative Colitis1,2
- Rectal pain, with or without diarrhoea
- Bloody diarrhoea
- Rectal bleeding
- Faecal incontinence
- Urgency / tenesmus
- Nocturnal defecation
- Abdominal cramps or pain
- Increased frequency of bowel movements

Crohn’s Disease3
- Abdominal pain often found in the lower right quadrant
- Chronic diarrhoea that can alternate with episodes of constipation
- Rectal bleeding or bloody diarrhoea
- Nausea / vomiting
- Ungaro R, et al. Lancet. 2017;389(10080):1756–1770.
- Magro F, et al. J Crohns Colitis. 2017;11(6):649–670.
- Torres J, et al. Lancet. 2017;389(10080):1741–1755.
Why are you at risk?
If you have IBD of any kind, you are at risk of iron deficiency. Learn more about the risk of IDA.


- WGO Global Guidelines. 2015
- Ng SC et al. Lancet. 2017;390:2769–2778
- Wilhelm SM and Bryan L. Clinical Pharmacist. 2017;Vol 9(3):online. DOI: 10.1211/CP.2017.20202316
- Burisch J et al. J Crohns Colitis. 2013;7(4):322–337
- Kaser A et al. Annu Rev Immunol. 2010;28:573–621
- Guan Q. J Immunol Res. 2019;2019:7247238
- Kim DH and Cheon JH. Immune Network. 2017;17(1):25–40
- WGO Global Guidelines. 2015
- Rowe WA. Inflammatory Bowel Disease: Practice Essentials, Background, Pathophysiology. Medscape. 2017
- Stein J, Hartmann F, Dignass AU. Diagnosis and management of iron deficiency anemia in patients with IBD. Nat Rev Gastroenterol Hepatol. 2010;7(11):599-610. doi:10.1038/nrgastro.2010.151.
Αν έχετε οποιασδήποτε μορφής φλεγμονώδη νόσο του εντέρου, υπάρχουν μεγαλύτερες πιθανότητες να εμφανίσετε έλλειψη σιδήρου. Το 36%-76% περίπου των ατόμων με φλεγμονώδη νόσο του εντέρου εκδηλώνει σιδηροπενική αναιμία. Μάθετε περισσότερα για τη σιδηροπενική αναιμία.
Η έλλειψη σιδήρου μπορεί να επηρεάσει πολλά μέρη του σώματος. Μπορεί να εμφανίσετε ταυτόχρονα ένα ή περισσότερα από τα παρακάτω συμπτώματα. Δείτε αναλυτικά όλα τα σημάδια της έλλειψης σιδήρου.
Αν έχετε διαγνωστεί με φλεγμονώδη νόσο του εντέρου, πιθανότατα θα επισκέπτεστε τακτικά τον γιατρό που σας παρακολουθεί. Αν νιώθετε κόπωση ή έχετε τυχόν άλλα σημάδια έλλειψης σιδήρου, όπως χλωμή όψη, τάση για λιποθυμία ή ταχυκαρδία, θα ήταν καλό να μιλήσετε στον γιατρό σας για τα συμπτώματα αυτά και την έλλειψη σιδήρου. Θα ήταν χρήσιμο να σκεφτείτε τις πληροφορίες που ενδέχεται να χρειαστεί ο γιατρός σας για να διαπιστώσει την αιτία των συμπτωμάτων σας. Ο γιατρός μπορεί να πραγματοποιήσει εξετάσεις αίματος για να ελέγξει τα επίπεδα σιδήρου σας, πριν σας συστήσει κάποια θεραπεία για τη βελτίωσή τους.
Μετά την εξέταση των επιπέδων σιδήρου, ο γιατρός σας θα μπορεί να αποφασίσει ποια είναι η καλύτερη θεραπεία για εσάς. Αυτή θα εξαρτηθεί από τον βαθμό έλλειψης σιδήρου και μπορεί να περιλαμβάνει συμβουλές για το πώς μπορείτε να λαμβάνετε περισσότερο σίδηρο από τη διατροφή σας ή/και συστάσεις για φάρμακα που μπορείτε να πάρετε για τη βελτίωση των επιπέδων σιδήρου. Περισσότερες πληροφορίες υπάρχουν στον παρακάτω σύνδεσμο.
Αν έχετε οποιασδήποτε μορφής φλεγμονώδη νόσο του εντέρου, υπάρχουν μεγαλύτερες πιθανότητες να εμφανίσετε έλλειψη σιδήρου. Το 36%-76% περίπου των ατόμων με φλεγμονώδη νόσο του εντέρου εκδηλώνει σιδηροπενική αναιμία. Μάθετε περισσότερα για τη σιδηροπενική αναιμία.
Η έλλειψη σιδήρου μπορεί να επηρεάσει πολλά μέρη του σώματος. Μπορεί να εμφανίσετε ταυτόχρονα ένα ή περισσότερα από τα παρακάτω συμπτώματα. Δείτε αναλυτικά όλα τα σημάδια της έλλειψης σιδήρου.
Αν έχετε διαγνωστεί με φλεγμονώδη νόσο του εντέρου, πιθανότατα θα επισκέπτεστε τακτικά τον γιατρό που σας παρακολουθεί. Αν νιώθετε κόπωση ή έχετε τυχόν άλλα σημάδια έλλειψης σιδήρου, όπως χλωμή όψη, τάση για λιποθυμία ή ταχυκαρδία, θα ήταν καλό να μιλήσετε στον γιατρό σας για τα συμπτώματα αυτά και την έλλειψη σιδήρου. Θα ήταν χρήσιμο να σκεφτείτε τις πληροφορίες που ενδέχεται να χρειαστεί ο γιατρός σας για να διαπιστώσει την αιτία των συμπτωμάτων σας. Ο γιατρός μπορεί να πραγματοποιήσει εξετάσεις αίματος για να ελέγξει τα επίπεδα σιδήρου σας, πριν σας συστήσει κάποια θεραπεία για τη βελτίωσή τους.
Μετά την εξέταση των επιπέδων σιδήρου, ο γιατρός σας θα μπορεί να αποφασίσει ποια είναι η καλύτερη θεραπεία για εσάς. Αυτή θα εξαρτηθεί από τον βαθμό έλλειψης σιδήρου και μπορεί να περιλαμβάνει συμβουλές για το πώς μπορείτε να λαμβάνετε περισσότερο σίδηρο από τη διατροφή σας ή/και συστάσεις για φάρμακα που μπορείτε να πάρετε για τη βελτίωση των επιπέδων σιδήρου. Περισσότερες πληροφορίες υπάρχουν στον παρακάτω σύνδεσμο.